

Abstract
Introduction
Adult T-cell leukemia/lymphoma (ATLL) is a rare, aggressive T cell neoplasm associated with a retrovirus human T cell lymphotropic virus (HTLV-1) and carries a dismal prognosis. Within the United States, New York, and Florida see the majority of cases due to the concentration of Caribbean immigrants (Zell, Assal et al. 2016, Malpica, Pimentel et al. 2018). SEER data does not include states like New York and Florida where most cases are seen and therefore a true estimate of the disease burden in this country is not known (Chihara, Ito et al. 2012, Adams, Newcomb et al. 2016).
Aim
We aim to study the epidemiology and clinical outcomes of ATLL in the United States particularly in the state of New York.
Methods
Data for New York was obtained from the New York State Cancer Registry (NYSCR). Data were also retrieved from 18 Surveillance, Epidemiology, and End Results (SEER) registries in the United States. Patients with ATLL (HTLV-1 positive) (includes all variants) were categorized using the International Classification of Diseases for Oncology, Third Edition codes ICD-O-3 as 9827/3.
Race/ethnicity was categorized as non-Hispanic white, non-Hispanic black, all Hispanic and other/unknown in the NYSCR whereas it was categorized as non-Hispanic white, non-Hispanic black, all Hispanic, non-Hispanic American Indian/Alaska Native, non-Hispanic Asian or Pacific Islander, and non-Hispanic unknown race in SEER.
ATLL patients ≥ 15 years of age were identified from 1995 to 2014 in SEER and all ages were included in NYSCR. Survival was estimated from SEER follow-up data with Kaplan Meier survival analysis.
For NYSCR mean and median survival time (month) for deceased patients - cases diagnosed through death certificate only were removed. NYSCR does not conduct active patient follow-up and assumes patients are still alive if we didn't find a deathmatch through vital record or National Death Index linkages.
Results
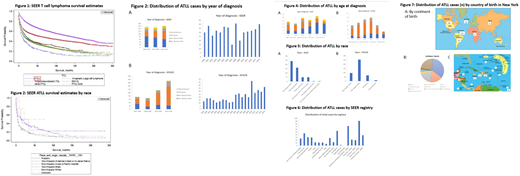
Five hundred and eleven patients with ATLL were identified in SEER. These patients had a median survival of 8 months (m) which was worse than all other subtypes of peripheral T cell lymphoma. (Figure 1) Four hundred and twenty-nine patients with ATLL were identified in NYSCR and these patients had a median survival of 4.5 m. (Figure 2)
Over the years from 2000 until 2014 the number of cases diagnosed within SEER registry coverage areas has not changed. In New York state however there has been a doubling in the number of cases diagnosed from 1995 to 2014. (Figure 3A, B)
The non-Hispanic black population was diagnosed at a median age of 52.5 in SEER and 54 in NYSCR while the non-Hispanic whites were diagnosed at a median age of 71 in SEER and 64.5 in NYSCR. The Hispanic patients were diagnosed at a median age of 58.5 in NYSCR and 52.5 in SEER. (Figure 4A, B) There was no gender predominance with 50% males in both registries.
ATLL patients in SEER were 47.2% non-Hispanic white, 31.7% non-Hispanic black, 9.8% Hispanic and 11.4% other/unknown. There were 5.5% Japanese patients (n=28) diagnosed in SEER. NYSCR had 22.4% non-Hispanic white, 59.4% non-Hispanic black, 15.9% Hispanic and 2.3% other/unknown. (Figure 5A, B)
Within SEER registries most cases occurred in New Jersey, California, Connecticut and Georgia. (Figure 6) New York state had a significantly higher number of cases than these states. Seventy four percent cases diagnosed within New York state are diagnosed in New York city and only 26% of cases are diagnosed in upstate New York.
Based on reported country of birth within New York state, only 27% of the ATLL cases diagnosed are born in the US whereas 49% are born in the Caribbean (most likely to be from Jamaica, Dominican Republic and Haiti). (Figure 7A, B, C)
For SEER and NYSCR the age-adjusted cancer incidence rate by race year and other factors will be presented at the meeting.
Conclusions
ATLL has a worse prognosis than all other PTCL subtypes. New York State has a high endemicity for ATLL with a rising number of cases. The higher percentage of non-Hispanic black patients in New York compared to the rest of the country is consistent with the diverse racial demographics in this state. Survival varied significantly by race/ethnicity and disparities were evident especially for non-Hispanic blacks who were diagnosed at a younger median age and had a shorter survival. Further research into this aggressive disease is needed to improve outcomes for these patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal